Careful Administration: Prevacid should be administered with caution to the following patients: Patients with a history of drug hypersensitivity; elderly patients (see Use in the elderly as follows); patients with impaired hepatic function (see Hepatic Impairment as follows).
Tablet: Presence of Gastric Malignancy: In adults, symptomatic response to therapy with PREVACID does not preclude the presence of gastric malignancy. Consider additional follow-up and diagnostic testing in adult patients who have a suboptimal response on an early symptomatic relapse after completing treatment with a PPI. In older patients, also consider an endoscopy.
Acute Interstitial Nephritis: Acute interstitial nephritis has been observed in patients taking PPIs including PREVACID. Acute interstitial nephritis may occur at any point during PPI therapy and is generally attributed to an idiopathic hypersensitivity reaction. Discontinue PREVACID if acute interstitial nephritis develops.
Cyanocobalamin (vitamin B12) Deficiency: Daily treatment with any acid-suppressing medications over a long period of time (e.g., longer than 3 years) may lead to malabsorption of cyanocobalamin (vitamin B12) caused by hypo- or achlorhydria. Rare reports of cyanocobalamin deficiency occurring with acid-suppressing therapy have been reported in the literature. This diagnosis should be considered if clinical symptoms consistent with cyanocobalamin deficiency are observed in patients treated with PREVACID.
Clostridium difficile Associated Diarrhea: Published observational studies suggest that PPI therapy like PREVACID may be associated with an increased risk of
Clostridium difficile-associated diarrhea (CDAD), especially in hospitalized patients. This diagnosis should be considered for diarrhea that does not improve.
Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated.
CDAD has been reported with use of nearly all antibacterial agents. For more information specific to antibacterial agents (clarithromycin and amoxicillin) indicated for use in combination with PREVACID, refer to Warnings and Precautions section of their prescribing information.
Bone Fracture: Several published observational studies suggest that proton pump inhibitor (PPI) therapy may be associated with an increased risk for osteoporosis-related fractures of the hip, wrist or spine. The risk of fracture was increased in patients who received high-dose, defined as multiple daily doses, and long-term PPI therapy (a year or longer). Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated. Patients at risk for osteoporosis-related fractures should be managed according to established treatment guidelines (see Dosage & Administration).
Hypomagnesemia: Hypomagnesemia, symptomatic and asymptomatic, has been reported rarely in patients treated with PPIs for at least three months, in most cases after a year of therapy. Serious adverse events include tetany, arrhythmias, and seizures. In most patients, treatment of hypomagnesemia required magnesium replacement and discontinuation of the PPI.
For patients expected to be on prolonged treatment or who take PPIs with medications such as digoxin or drugs that may cause hypomagnesemia (e.g., diuretics), healthcare professionals may consider monitoring magnesium levels prior to initiation of PPI treatment and periodically.
Interaction with Methotrexate: Literature suggests that concomitant use of PPIs with methotrexate (primarily at high dose may elevate and prolong serum levels of methotrexate and/or its metabolite, possibly leading to methotrexate toxicities. In high-dose methotrexate administration, a temporary withdrawal of the PPI may be considered in some patients (see Interactions).
Cutaneous and Systemic Lupus Erythematosus: Cutaneous lupus erythematosus (CLE) and systemic lupus erythematosus (SLE) have been reported in patients taking PPIs, including lansoprazole. These events have occurred as both new onset and an exacerbation of existing autoimmune disease. The majority of PPI-induced lupus erythematosus cases were CLE.
The most common form of CLE reported in patients treated with PPIs was subacute CLE (SCLE) and occurred within weeks to years after continuous drug therapy in patients ranging from infants to the elderly. Generally, histological findings were observed without organ involvement.
Systemic lupus erythematosus (SLE) is less commonly reported than CLE in patients receiving PPIs. PPI associated SLE is usually milder than non-drug induced SLE. Onset of SLE typically occurred within days to years after initiating treatment primarily in patients ranging from young adults to the elderly. The majority of patients presented with rash; however, arthralgia and cytopenia were also reported.
Avoid administration of PPIs for longer than medically indicated. If signs or symptoms consistent with CLE or SLE are noted in patients receiving PREVACID, discontinue the drug and refer the patient to the appropriate specialist for evaluation. Most patients improve with discontinuation of the PPI alone in four to 12 weeks.
Serological testing (e.g., ANA) may be positive and elevated serological test results may take longer to resolve than clinical manifestations.
Interactions with Investigations for Neuroendocrine Tumors: Serum chromogranin A (CgA) levels increase secondary to drug-induced decreases in gastric acidity. The increased CgA level may cause false positive results in diagnostic investigations for neuroendocrine tumors. Healthcare providers should temporarily stop lansoprazole treatment at least 14 days before assessing CgA levels and consider repeating the test if initial CgA levels are high. If serial tests are performed (e.g., for monitoring), the same commercial laboratory should be used for testing, as reference ranges between tests may vary (see Interactions).
Patients with Phenylketonuria: Phenylalanine can be harmful to patients with phenylketonuria (PKU). PREVACID FDT contains phenylalanine, a component of aspartame. Each 15 mg tablet contains 2.5 mg and each 30 mg tablet contains 5.1 mg of phenylalanine. Before prescribing PREVACID FDT to a patient with PKU, consider the combined daily amount of phenylalanine from all sources, including PREVACID FDT.
Hepatic Impairment: In patients with various degrees of chronic hepatic impairment the exposure to lansoprazole was increased compared to healthy subjects with normal hepatic function. No dosage adjustment for PREVACID is necessary for patients with mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment. The recommended dosage is 15 mg orally daily in patients with severe hepatic impairment (Child-Pugh Class C).
IV: Important Precautions: As PREVACID I.V. was shown to have high hemostatic effect based on the data up to 3 days after starting treatment, once the patient is able to take medications orally, therapy should be switched to an oral formulation and this drug should not be administered aimlessly for a long period (see Pharmacology: Pharmacodynamics: Clinical Studies under Actions).
There is no clinical experience of treatment over 7 days in Japanese clinical trials.
At the treatment, the course of the disease should be closely observed and the minimum therapeutic necessity should be used according to the disease condition. If PREVACID I.V. is ineffective, it should be switched to another treatment.
If the patient has projectile bleeding or oozing bleeding, or is considered at risk for rapid bleeding such as the case of presence of exposed blood vessels, the patient should undergo endoscopic hemostasis such as heater probe or clipping.
Other Precautions: In an animal study in which 50 mg/kg/day (about 100 times the clinical dose) of lansoprazole was given to rats by gavage administration for 52 weeks, benign testicularinterstitial cell tumors were observed in one animal. In another study in which 15 mg/kg/day or more was given to rats by gavage for 24 months, an increase in the frequency of benign testicular interstitial cell tumors was observed and, in which 5 mg/kg/day or more was given, carcinoid tumors in the stomach were observed. In addition, in the group of female rats given 15 mg/kg/day or more of lansoprazole and the group of male rats given 50 mg/kg/day or more, an increase in the frequency of retinal atrophy was observed. Testicular interstitial cell tumors and retinal atrophy were not observed in carcinogenicity studies in mice, as well as in toxicity studies in dogs or monkeys. Thus, these changes are considered to be specific to rats.
The administration of PREVACID I.V. may mask the symptoms of gastric cancer. It is, therefore, necessary to ascertain the ulcer is not of a malignant nature before initiating the administration of this drug.
In several observational studies in overseas, an increased risk for osteoporosis-related fractures of the hip, wrist or spine under the treatment with proton pump inhibitors has been reported. The risk of fracture was especially increased in the patients receiving high dose or long term (a year or longer) treatment.
In several overseas observational studies, mainly in hospitalized patients, increased risk of gastrointestinal infection caused by
Clostridium difficile was reported in patients received proton pump inhibitors.
Cyanocobalamin (Vitmain B-12) Deficiency: Daily treatment with any acid-suppressing medications over a long period of time (e.g., longer than three years) may lead to malabsorption of cyanocobalamin (Vitamin B-12) caused by hypo- or achlorhydria. Rare reports of cyanocobalamin deficiency occurring with acid-suppressing therapy have been reported in the literature. This diagnosis should be considered if clinical symptoms consistent with cyanocobalamin deficiency are observed.
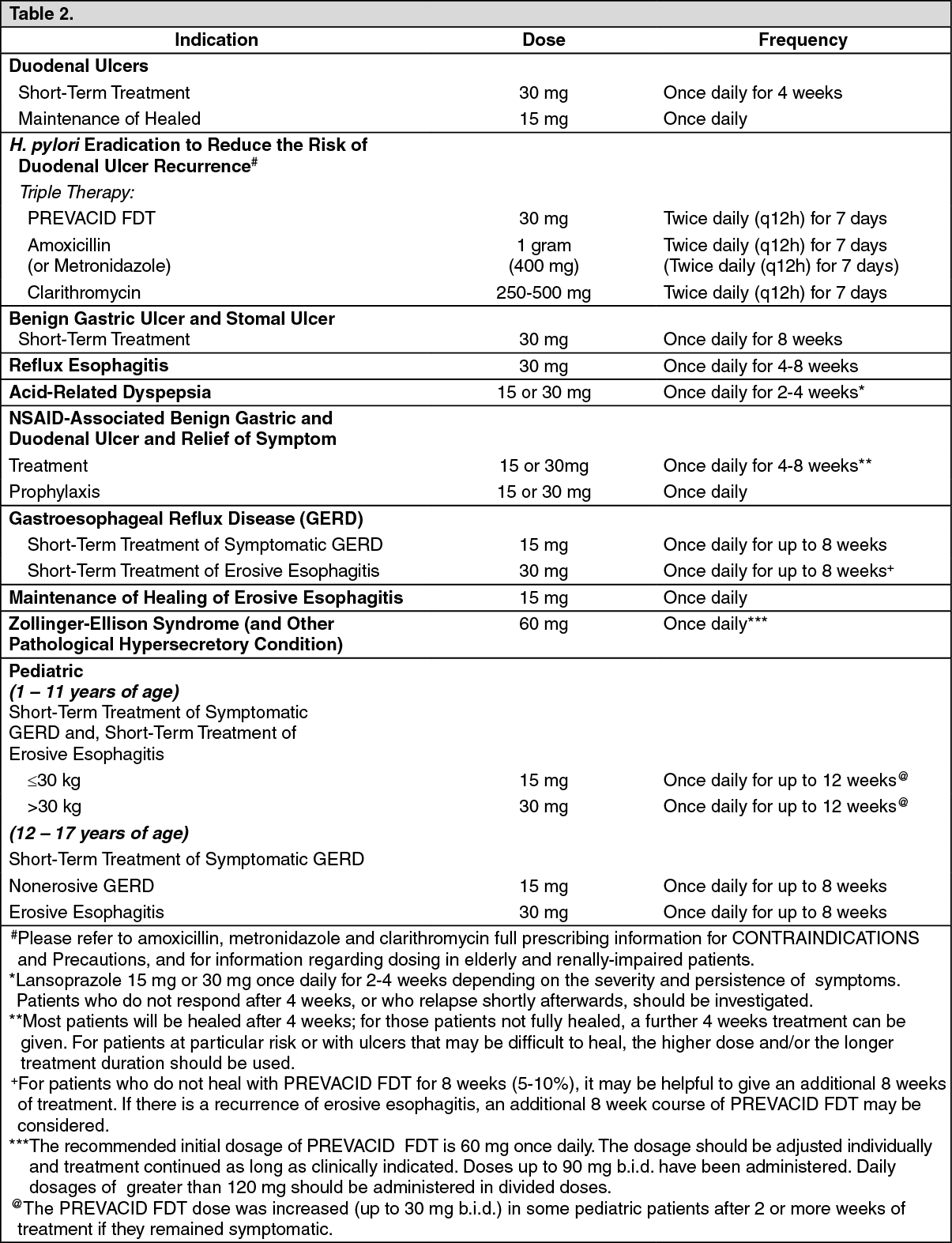
Use in Children: Tablet: The safety and effectiveness of PREVACID FDT have been established in pediatric patients one to 17 years of age for short-term treatment of symptomatic GERD and erosive esophagitis, however, lansoprazole was not effective in patients with symptomatic GERD 1 month to less than one year of age in a multi-center, double-blind, placebo controlled study.
Use of PREVACID FDT in this population is supported by evidence from adequate and well controlled studies of PREVACID FDT in adults with additional clinical, pharmacokinetic, and pharmacodynamic studies performed in pediatric patients. The adverse events profile in pediatric patients is similar to that of adults. There were no adverse events reported in U.S. clinical studies that were not previously observed in adults.
Neonate to less than 1 year of age: The pharmacokinetics of lansoprazole were studied in pediatric patients with GERD aged less than 28 days and 1 to 11 months. Compared to healthy adults receiving 30 mg, neonates had higher exposure (mean weight-based normalized AUC values 2.04- and 1.88-fold higher at doses of 0.5 and 1 mg/kg/day, respectively). Infants aged ≤10 weeks had clearance and exposure values that were similar to neonates. Infants aged greater than 10 weeks who received 1 mg/kg/day had mean AUC values that were similar to adults who received a 30 mg dose.
Lansoprazole was not found to be effective in a U.S. and Polish 4 week multi-center, double-blind, placebo-controlled, parallel-group study of 162 patients between one month and less than 12 months of age with symptomatic GERD based on a medical history of crying/fussing/irritability associated with feedings who had not responded to conservative GERD management (i.e., non-pharmacologic intervention) for 7 to 14 days. Patients received lansoprazole as a suspension daily (0.2 to 0.3 mg/kg/day in infants ≤10 weeks of age or 1.0 to 1.5 mg/kg/day in infants greater than 10 weeks or placebo) for up to 4 weeks of double-blind treatment.
The primary efficacy endpoint was assessed by greater than 50% reduction from baseline in either the percent of feedings with a crying/fussing/irritability episode or the duration (minutes) of a crying/fussing/irritability episode within one hour after feeding.
There was no difference in the percentage of responders between the lansoprazole pediatric suspension group and placebo group (54% in both groups).
There were no adverse events reported in pediatric clinical studies (one month to less than 12 months of age) that were not previously observed in adults.
Based on the results of the Phase 3 efficacy study, lansoprazole was not shown to be effective. Therefore, these results do not support the use of lansoprazole in treating symptomatic GERD in infants.
1 to 11 years of age: In an uncontrolled, open label, U.S. multi-center study, 66 pediatric patients (1 to 11 years of age) with GERD were assigned, based on body weight, to receive an initial dose of either PREVACID FDT 15 mg q.d. if ≤ 30 kg or PREVACID FDT 30 mg q.d. if > 30 kg administered for 8 to 12 weeks. The PREVACID FDT dose was increased (up to 30 mg b.i.d.) in 24 of 66 pediatric patients after 2 or more weeks of treatment if they remained symptomatic. At baseline 85% of patients had mild to moderate overall GERD symptoms (assessed by investigator interview), 58% had non-erosive GERD and 42% had erosive esophagitis (assessed by endoscopy).
After 8 to 12 weeks of PREVACID FDT treatment, the intent-to-treat analysis demonstrated an approximate 50% reduction in frequency and severity of GERD symptoms.
Twenty-one of 27 erosive esophagitis patients were healed at 8 weeks and 100% of patients were healed at 12 weeks by endoscopy. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a study of 66 pediatric patients in the age group 1 year to 11 years old after treatment with PREVACID FDT given orally in doses of 15 mg q.d. to 30 mg b.i.d., increases in serum gastrin levels were similar to those observed in adult studies. Median fasting serum gastrin levels increased 89% from 51 pg/ml at baseline to 97 pg/ml [interquartile range (25
th-75
th percentile) of 71-130 pg/ml] at the final visit.
The most frequently reported (2 or more patients) treatment-related adverse events in patients 1 to 11 years of age (N=66) were constipation (5%) and headache (3%).
12 to 17 years of age: In an uncontrolled, open-label, U.S. multi-center study, 87 adolescent patients (12-17 years of age) with symptomatic GERD were treated with PREVACID FDT for 8 to 12 weeks. Baseline upper endoscopies classified these patients into two groups: 64 (74%) non-erosive GERD and 23 (26%) erosive esophagitis (EE). The non-erosive GERD patients received PREVACID FDT 15 mg q.d. for 8 weeks and the EE patients received PREVACID FDT 30 mg q.d. for 8 to 12 weeks. At baseline, 89% of these patients had mild to moderate overall GERD symptoms (assessed by investigator interviews). During 8 weeks of PREVACID FDT treatment, adolescent patients experienced a 63% reduction in frequency and a 69% reduction in severity of GERD symptoms based on diary results.
Twenty-one of 22 (95.5%) adolescent erosive esophagitis patients were healed after 8 weeks of PREVACID FDT treatment. One patient remained unhealed after 12 weeks of treatment. (See Table 4.)
Click on icon to see table/diagram/image
In these 87 adolescent patients, increases in serum gastrin levels were similar to those-observed in adult studies, median fasting serum gastrin levels increased 42% from 45 pg/ml at baseline to 64 pg/ml [interquartile range (25
th - 75
th percentile) of 44 - 88 pg/ml] at the final visit. (Normal serum gastrin levels are 25 to 111 pg/ml).
The most frequently reported (at least 3%) treatment-related adverse events in these patients were headache (7%), abdominal pain (5%), nausea (3%) and dizziness (3%). Treatment-related dizziness, reported in this prescribing information as occurring in <1% of adult patients, was reported in this study by 3 adolescent patients with non-erosive GERD, who had dizziness concurrently with other events (such as migraine, dyspnea, and vomiting).
IV: The safety of PREVACID I.V. in children has not been established (no clinical experience).
Use in the Elderly: Tablet: Of the total number of patients (n=21,486) in clinical studies of PREVACID, 16% of patients were aged 65 years and over, while 4% were 75 years and over. No overall differences in safety or effectiveness were observed between these patients and younger patients and other reported clinical experience has not identified significant differences in responses between geriatric and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
IV: Since physiological function is generally decreased in elderly patients, PREVACID I.V. should be carefully administered.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image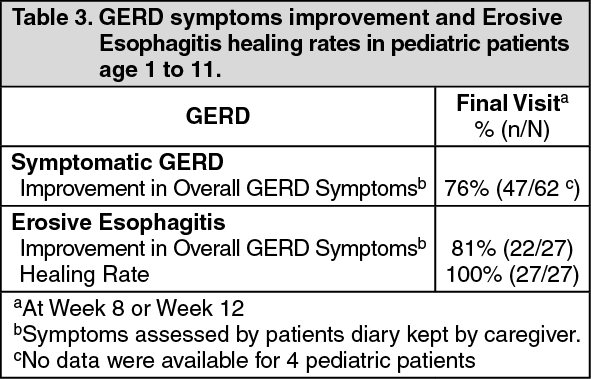 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image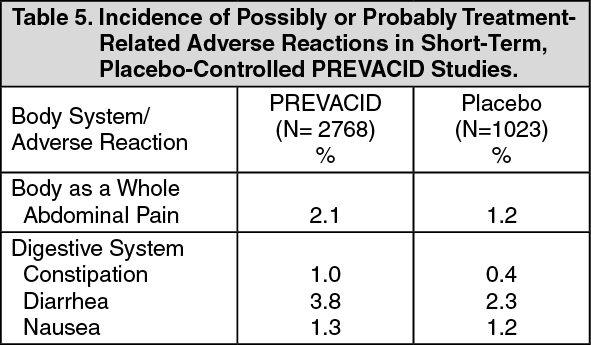 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image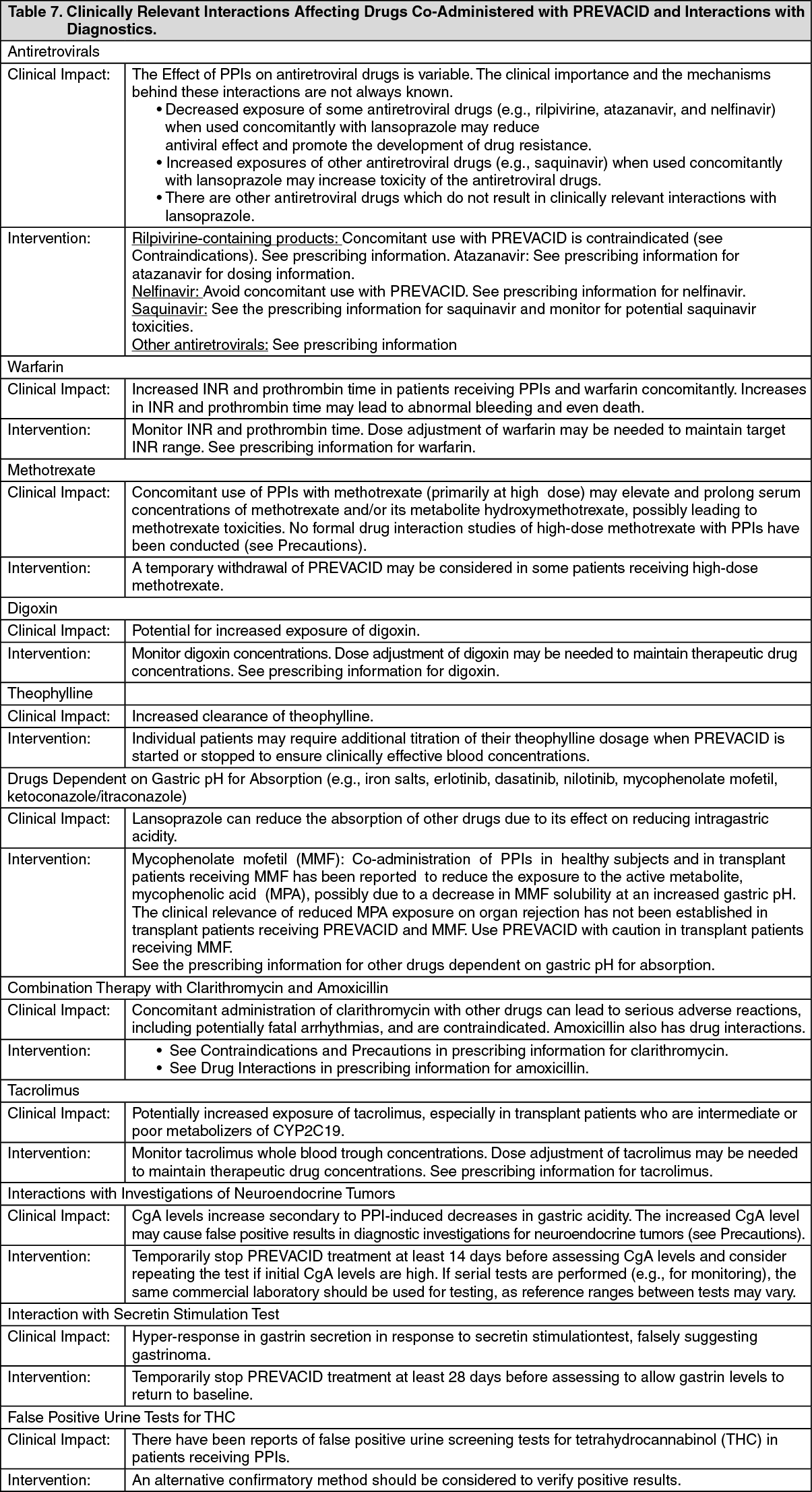 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
